KDVS FAQ
Genetics is a complex and quickly advancing field and as such, there are no simple explanations. We encourage you to speak with your geneticists and genetic counselors with additional questions or to help explain these complex subjects.
Koolen-de Vries Syndrome Foundation thanks our Medical Advisory Board for providing answers to these Frequently Asked Questions.
Disclaimer: These questions are meant to address common inquiries about Koolen-de Vries Syndrome. Koolen-de Vries Syndrome Foundation is not giving medical advice or guidance by answering these questions. Each individual with Koolen-de Vries Syndrome may experience unique symptoms or have a different medical history that other individuals.
Are there any known differences between the presentation of the microdeletion and the KANSL1 mutation at this time (2015)?
KdVS caused by a mutation in the KANSL1 gene is very rare. Based on relatively small numbers there doesn’t seem to be a difference between the presentation of the 17q21.31 deletion and the KANSL1 mutation.
Does the size of the microdeletion or the number of genes deleted affect the severity of symptoms?
The size of most 17q21.31 deletions are almost identical and the severity of the symptoms is probably caused by other (genetic) factors.
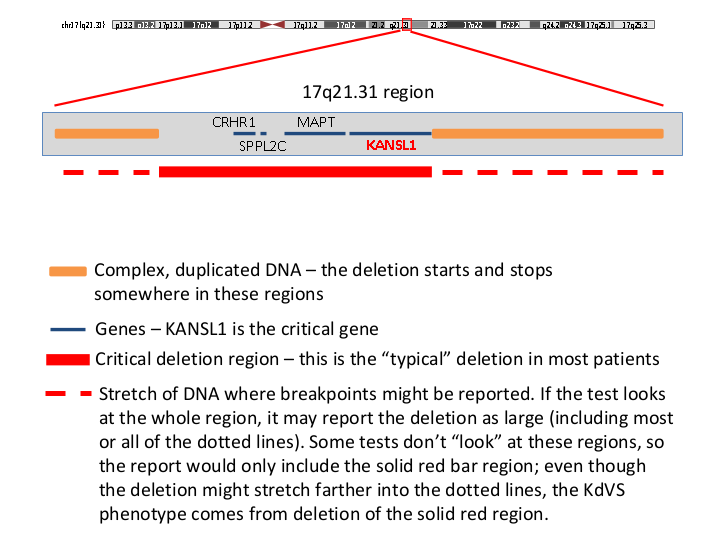
KdVS can be caused by the fact that a small part of chromosome 17 is missing (17q21.31 deletion). The 17q21.31 region is a very complicated region in the human DNA and can harbor blocks of repetitive DNA (orange in the Figure below) that are almost identical. Because of these blocks of DNA, the region is vulnerable for deletions to occur. The breakpoints of almost all 17q21.31 deletion reside within the blocks of repetitive DNA. In other words, all deletions are almost identical.
Still, the array results show differently. Sometimes there seems to be a relatively large difference in the size of the deletions. It is questionable whether that is actually the case. The different array platforms are not very accurate in defining the deletion breakpoints at the base pair level, especially within the repetitive DNA blocks. Probably, the deletions are very similar if the breakpoints and the deletion size are established using other techniques. This is not possible in a diagnostic setting. On the other hand, it is also not necessary. The typical 17q21.31 deletion (solid red bar) always includes (part of) the KANSL1 gene and it has been shown that a defect of the KANSL1 gene is the main cause of the KdVS.
If a child is found to have the microdeletion or the mutation – what reasons might a parent have to also have genetic testing? Which tests should the parent have? Is there any reason a sibling should be tested?
Testing for the H2 17q21.31 inversion is not warranted in a clinical setting.
We test the parents of a child with a typical 17q21.31 deletion, although the clinical relevance is limited. FISH for the 17q21.31 region in the parents can be considered in order to test for mosaicism in one of the parents. This might be helpful especially if the parents want to know their individual chance of having another child with KdVS. We described two independent families with both two boys with KdVS. In both families one of the parents had the 17q21.31 deletion in a low percentage of the cells that were tested. That is called mosaicism. For these parents the chance in future pregnancies is markedly increased. Mosaicism is rare and although FISH can be helpful, mosaicism can never be excluded.
The parents of a child with a KANLS1 mutation always have to be tested. Not every change in the nucleotides at the gene level disturbs the function of the gene. Moreover, part of the gene is copied and the mutation might be in the pseudogene. Testing the parents by sequencing the KANSL1 gene is essential for the clinical interpretation of the result. If a mutation is also found in one of the parents the diagnosis of KdVS should be questioned.
In case of a deletion or KANSL1 mutation that is not found in one of the parents, brothers or sisters without any signs of KdVS should not be tested. For them there is not an increased chance of having a child with KdVS.
I hear people talk about the inversion. What does that mean? Does one of the parents of an individual with KDVS have to have the inversion? Is there a way to test for the inversion – or is that necessary? If you do have the inversion, does it mean you are more likely to have another KDVS child?
The 17q21.31 region is a complex region in the human DNA. For example, part of the 17q21.31 region can be inverted. This inversion is called the H2 lineage. An inversion means that a part of chromosome has been broken twice, flipped 180 degrees, and rejoined. This inversion has been around for millions of years. The H2 lineage is not only inverted but there are also some other differences with the H1 lineage.
The H1 lineage is more common than the H2 lineage, but we have seen that at least one of the parents of a child with a 17q21.31 deletion has the H2 inversion. We concluded that the H2 inversion is a necessary factor for the deletion to occur. That is explained by the following:
The cause of KdVS in most children is the loss of a small part of chromosome 17 (17q21.31 microdeletion) including the gene called KANSL1. At either side of the region that is missing in the syndrome there are DNA stretches that are very similar (so called low copy repeats). This might result in the deletion during the formation of the sperm cells or the formation of the egg cells by a mechanism called non-allelic homologous recombination (NAHR).
For NAHR to result in a deletion of the region in between, the pieces of (almost) identical DNA have to be in the same direction and that is only the case in the H2 lineage. That’s why the deletion only occurs if at least one of the parents has an 17q21.31 inversion.
However, the chance of having a H2 inversion in the Caucasian population is 40%. Therefore, many other factors are also important. All parents of a child with KdVS have a higher chance of having another child with KdVS compared to the general population, but in general, this chance for future pregnancies is relatively low (probably less than 1%). Testing for the inversion does not provide additional information that is of clinical use.
Please explain how the 17q21.31 microdeletion is found using genetic testing (FISH vs microarry)? Please explain what testing finds the mutation that causes Koolen-de Vries Syndrome?
Most 17q21.31 deletions will be identified by microarray analysis. Microarrays test all chromosomes for changes in copy number. The technique can find pieces of DNA that are missing and pieces that are duplicated. The big advantage is that you don’t need to know what you are looking for in advance: all chromosomes are testing with high resolution. FISH is a targeted technique. If the clinician thinks of KdVS because of some clinical features, they might perform FISH analysis. The test will show whether the deletion is present or not.
The 17q21.31 deletion is about 500,000 nucleotides (DNA building blocks) in size. The deletion includes the KANLS1 gene. Children with KdVS because of a KANSL1 mutation do have two copies of the KANSL1 gene and the 17q21.31 region. However, one of the KANSL1 genes does not work, because of small changes at the nucleotide level. A single change in one nucleotide can disturb the function of KANSL1 and result in KdVS. FISH or microarrays cannot identify singe nucleotide changes. For the identification of these small changes Sanger sequencing of the KANSL1 gene is used or even whole exome/genome sequencing.